

Lapiplasty® Educational Video
Lapiplasty® Surgical Demonstration
Why perform the Lapiplasty® Procedure?
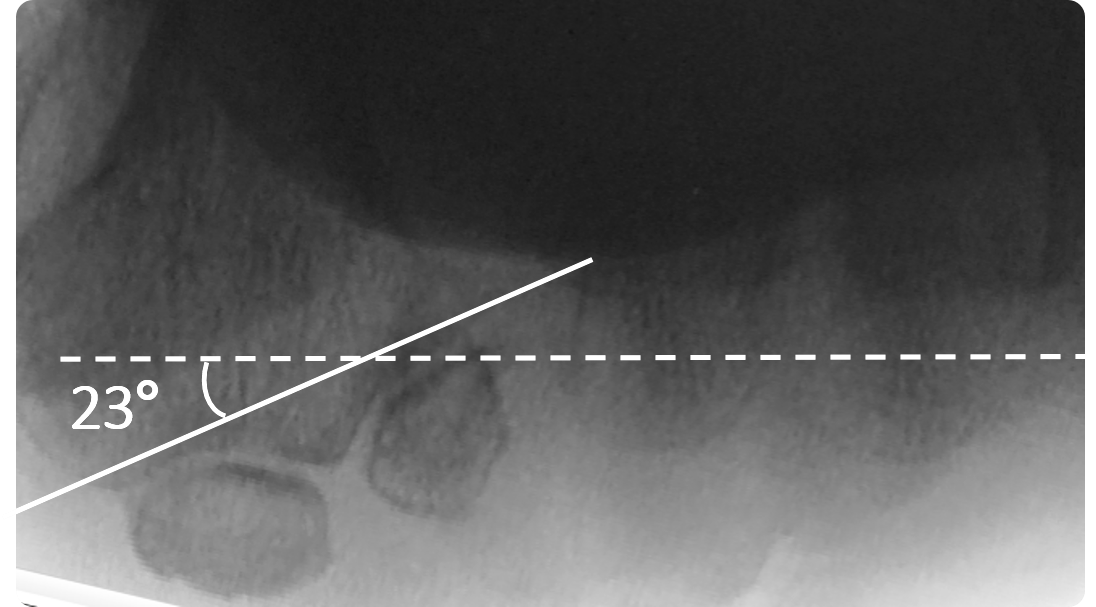
Because metatarsal frontal-plane rotation matters
While hallux valgus has traditionally been viewed as a transverse plane deformity, research indicates that it is actually a three-plane deformity with 87% of patients having abnormal frontal-plane rotation (i.e. pronation) of the 1st metatarsal.3 Correction of metatarsal rotation is critical for restoration of anatomic first ray alignment (MTP joint congruity and sesamoid position), which left unaddressed, is associated with up to 12x likelihood of radiographic recurrence.4,5,6 Due to the ability to address the triplanar deformity at its origin, the 1st tarsometarsal (TMT) joint provides the optimal surgical site for true anatomic restoration.Learn more about metatarsal frontal-plane rotation.

What is the Lapiplasty® Procedure?
An instrumented, reproducible approach to 3-plane correction with rapid return to weight-bearing7
Correct.
Make your correction before you cut
The Lapiplasty® Positioner is engineered to quickly and reproducibly correct the alignment in all three planes, establishing and holding true anatomic alignment of the metatarsal and sesamoids.8
Cut.
Perform precision cuts with confidence
The Lapiplasty® Cut Guide delivers precise cuts with the metatarsal held in the corrected position, ensuring optimal cut trajectory while virtually eliminating the risk of metatarsal shortening.
Compress.
Achieve controlled compression of joint surfaces
The Lapiplasty® Compressor delivers over 150N of controlled compression9 to the precision-cut joint surfaces, while maintaining the 3-plane correction.
Fixate.
Apply multiplanar fixation for robust stability
Low-profile Biplanar™ Plating provides biomechanically-tested 10,11 multiplanar stability for rapid return to weight-bearing.7
How does the Lapiplasty® Procedure work?
Key Surgical Steps*

1. Joint Release
Run sagittal saw cengruously down the 1st TMT joint to mobilize and plane the joint surfaces.
2. Anatomic Correction
Apply the Lapiplasty® Posltioner, simultaneously securing the IM angle, frontal-plane rotation, and sagittal alignment in corrected position.
3. Precision Cuts
Secure the Lapiplasty® Cut Guide and make precise joint cuts with the triplanar correction held In place.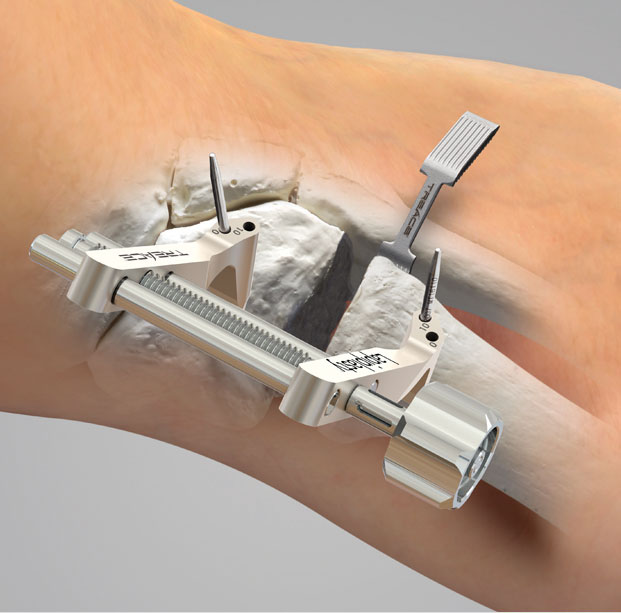
4. Joint Distraction
Apply the Lapiplasty® Compressor over the Cut Guide Pins to distract the joint for removal of bone slices and fenestration of the joint surfaces.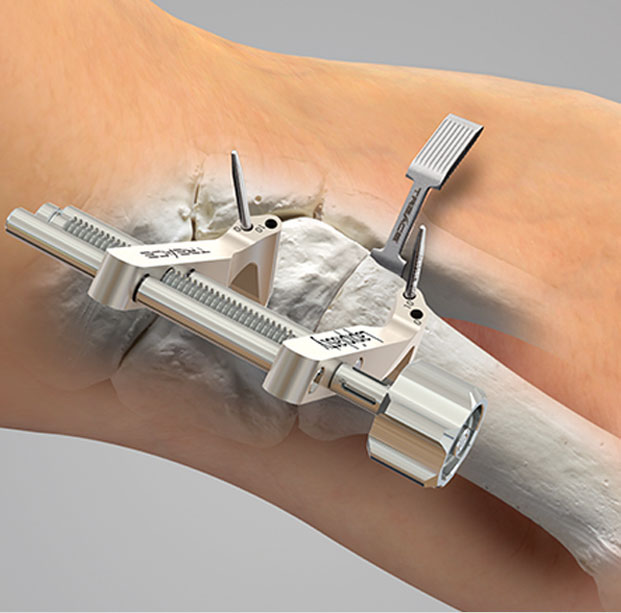
5. Joint Compression
Using·the Lapiplasty® Compressor, bring the precision-cut joint surfaces together for controlled apposition and compression of the arthrodesis site.
6. Multiplanar Fixation
Apply low-profile Biplanar™ Plates dorsally and medially, providing multiplanar fixation for rapid weight-bearing.* Treace Medical Concepts, Inc. Surgical Technique LBL 1405-9001
Covered by one of more patents. See www.treace.com/patients
Lapiplasty® System
Anatomic Biplanar™ Implants
Lapiplasty® System 1
Sterile-packed Biplanar™ Plating kit for versatility to fit each patient's anatomy, while delivering superior multiplanar strength.SK12

Lapiplasty® System 2
An evolution of Biplanar™ Plating with increased cross-sectional width and 2.7mm screws for additional construct strength.SK14

Lapiplasty® System 3R
Most robust Biplanar™ Plating option with widest cross-section, 3.0mm screws, and increased span to address revision cases and challenging anatomy.
Plantar Python® Plate
Sterile-packed for use with the Lapiplasty® System, the Platnar Python® Plate is uniquely pre-contoured for easy-to-apply tension-side fixation.S1: SD11/12 (L/R) S2: SD14/15 (L/R)

One System for All Your Hallux Valgus Needs
Sterile-packed kits for operational efficiency
Sterile-packed kits for operational efficiency
Lapiplasty® Compression Screws






Biomechanically Proven for Rapid Weight-Bearing
Biomechanical test specimens were constructed using Sawbones









The Evidence-Based Solution for 3-Plane Correction
Treace Medical Concepts is dedicated to advancing the understanding of the Lapiplasty® Procedure and its benefits to patients, surgeons, and the healthcare system through research studies and publications in the peer-reviewed literature.
Multicenter Early Radiographic Outcomes of Triplanar Tarsometatarsal Arthrodesis With Early Weightbearing
Multicenter, retrospective study of 57 hallux valgus (62 feet) patients treated with the Lapiplasty® Procedure and early return to weight-bearing at mean follow-up of 13.5 months.

Ray JJ, et al. Foot Ankle Int. 2019 [published online ahead of print]
- Mean return to weight-bearing at 10.9 days in a walking boot
- 96.8% of study patients maintained their 3-plane bunion correction as assessed by Intermetatarsal Angle (IMA), Hallux Valgus Angle (HVA) and Tibial Sesamoid Position (TSP)
- Symptomatic non-union rate of 1.6% (1 foot)
Progression of Healing on Serial Radiographs Following First Ray Arthrodesis in the Foot Using a Biplanar Plating Technique Without Compression
Multicenter, retrospective study of bone healing with accelerated weightbearing protocol in 195 patients undergoing TMT or MTP fusions with Lapiplasty® biplanar plating at mean follow up of 9.5 months.
Highlights of the study:- Patients began weight-bearing at 5 days post-op in a walking boot
- 97.4% of the patients demonstrated a successful bony fusion
- 98.9% of the patients maintained a stable joint position
- Ray JJ, et al. Multicenter Early Radiographic Outcomes of Triplanar Tarsometatarsal Arthrodesis With Early Weightbearing. Foot Ankle Int. 2019, [published online ahead of print].
- Dayton P, et al. Progression of Healing on Serial Radiographs Following First Ray Arthrodesis in the Foot Using a Biplanar Plating Technique Without Compression. Foot Ankle Surg. 2019, [published online ahead of print].
- Hatch et al. Triplane Hallux Abducto Valgus Classification. J Foot Ankle Surg. 2018, 57:972–981.
- Dayton et al. Biomechanical Characteristics of Biplane Multiplanar Tension-Side Fixation for Lapidus Fusion. J Foot Ankle Surg. 2018, 57:766-770.
- Dayton (Ed.) Evidence-Based Bunion Surgery: A Critical Examination of Current and Emerging Concepts and Techniques. Springer International Publishing [Textbook]. 2018.
- Santrock et al. Hallux Valgus Deformity and Treatment. A Three-Dimensional Approach: Modified Technique for Lapidus Procedure. Foot Ankle Clin. 2018, 23:281-295.
- Smith et al. Understanding Frontal Plane Correction in Hallux Valgus Repair. Clin Podiatr Med Surg. 2018, 35:27-36.
- Dayton et al. Comparison of Tibial Sesamoid Position on Anteroposterior and Axial Radiographs Before and After Triplane Tarsal Metatarsal Joint Arthrodesis. J Foot Ankle Surg. 2017, 56:1041-1046.
- Smith et al. Intraoperative Multiplanar Alignment System to Guide Triplanar Correction of Hallux Valgus Deformity. Techniques in Foot & Ankle Surgery. 2017, 16:175-82.
- Dayton et al. Comparison of the Mechanical Characteristics of a Universal Small Biplane Plating Technique Without Compression Screw and Single Anatomic Plate with Compression Screw. J Foot Ankle Surg. 2016, 55:567-71.
Learn more about the Lapiplasty® System components:



Lapiplasty® Resources
References
1Smith B, et al. 2017 AOFAS Annual Meeting, Seattle, WA.
2Ray JJ, et al. Foot Ankle Int. 2019.
3Kim Y, Kim JS, Young KW, et al. Foot Ankle Int. 2015, 36:944-52.
4Pentikainen I, Ojala R, Ohtonen P, et al. Foot Ankle Int. 2014, 35:1262-7.
5Okuda R, Kinoshita M, Yasuda T, et al. J Bone Joint Surg Am. 2009, 91:1637-4.
6Okuda R, Kinoshita M, Yasuda T, et al. J Bone Joint Surg Am. 2007, 89:2163-72.
7Smith B, et al. 2017 AOFAS Annual Meeting, Seattle, WA.
8Ray JJ, et al. Foot Ankle Int. 2019. (published online ahead of print)
9Data on file.
10Dayton P, et al. J Foot Ankle Surg. 2016. 55:567-71.
11Data on file.